

Anyone shopping for peptides to fight off infections runs into the same pitch fast: this one is antiviral, that one is the body’s “own” antimicrobial, take it and get sick less. The specificity sounds convincing, more convincing than the vague “boosts immunity” language that surrounds most supplements. But specificity and evidence are not the same thing, and a reader trying to sort one from the other has to separate two very different questions: which peptide has a real case, and where would anyone responsibly get it.
Most of what circulates under the “immune peptides” label, thymosin alpha-1, thymulin, LL-37, glutathione, VIP, is not FDA-approved for immune use in the United States. Some are compounded prescription products. Some are research-status compounds with no approved human use at all. That distinction matters more than any single ingredient name, and it’s the thread running through everything below.
The landscape: two peptides actually have a case
Narrow the category down to antimicrobial or antiviral defense specifically, and only two compounds are worth discussing seriously.
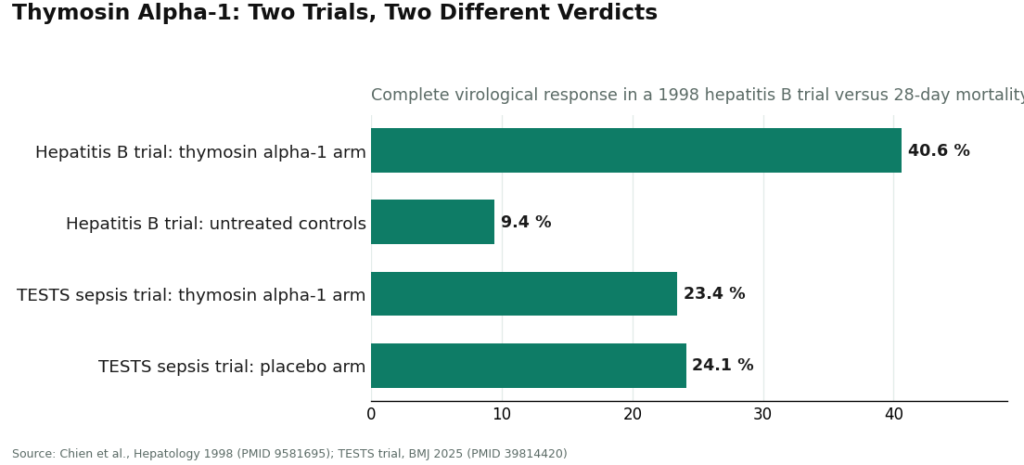
Thymosin alpha-1 has the deeper track record. The synthetic version is an approved drug in more than 35 countries, including for hepatitis B and C, and it functions as a TLR-2 and TLR-9 agonist that helps normalize T-cell activity [1]. A 1998 randomized controlled trial in 98 chronic hepatitis B patients backs that up in numbers: a 26-week course produced a complete virological response in 40.6% of treated patients versus 9.4% of untreated controls, and the study authors called it effective and safe [2].
That’s the good half of the story. The other half showed up when the trials got bigger and broader. The large, double-blind TESTS trial, run in 1,089 sepsis patients, found 28-day mortality of 23.4% in the thymosin alpha-1 group versus 24.1% on placebo, a difference small enough to call essentially none [3]. So the compound has a legitimate antiviral resume in a specific disease context, and it is not a general infection shield, whatever a sales page implies.
LL-37 is the trickier of the two, because the marketing writes itself: it’s the only human member of the cathelicidin family of antimicrobial peptides, doing genuine work in the body’s own defenses [4]. The best human evidence for it is topical. A randomized, placebo-controlled trial of topical LL-37 in 34 patients with hard-to-heal venous leg ulcers found it safe and effective at improving wound healing [5]. That’s a real, if narrow, result.
Push past topical use into the systemic, injected version that sellers hint at, and the evidence turns cautionary. Reviews of the cathelicidin family describe host-cell toxicity at higher concentrations, proteolytic instability, and a role as an autoantigen in autoimmune diseases like psoriasis and lupus [6]. Preclinical work has even raised the possibility that LL-37 could promote local invasion in melanoma by activating tumor cells and tumor-associated macrophages [7]. “The body’s own antimicrobial peptide” turns out to cut both ways, and the one solid clinical trial behind it is a wound-cream study, nowhere near the systemic use being implied elsewhere.
The tradeoffs: evidence versus access
Here’s where the category gets genuinely complicated, and where a shopper’s decision-making actually needs to happen.
The molecules with any real case are, not coincidentally, the ones you’d least want to buy carelessly. Thymosin alpha-1 is an injectable that’s approved abroad but not broadly in the US, which means the legitimate domestic path is a prescription filled through compounding, not a vial ordered from a chemical-supply site. LL-37’s mixed safety profile [6] is exactly the kind of thing that belongs in front of a clinician, not something to self-administer because a website described it cleanly.
The sourcing risk here isn’t theoretical. In 2019, the FDA warned compounders against making injectable glutathione from dietary-grade powder after a cluster of patient harm tied to laboratory-confirmed excessive endotoxin [8]. Glutathione isn’t even one of the two compounds under discussion here, but the warning is the clearest evidence available that, for injected products, the pharmacy behind the product is the safety story, not a footnote to it. A research-chemical vial offers no protection against that kind of failure, full stop.
So the practical tradeoff isn’t really “thymosin alpha-1 or LL-37.” It’s “supervised or unsupervised,” and that turns out to be the more consequential fork.
The shortlist, and the reasonable pick
Judged strictly on oversight, the field splits cleanly into two tiers.
| Provider | Model | Clinician + Rx? | Pharmacy | Honest about the evidence? |
|---|---|---|---|---|
| FormBlends | Licensed telehealth | Yes | Licensed 503A compounding | Yes, presents the evidence as uneven |
| HealthRX.com | Licensed telehealth | Yes | Pharmacy-dispensed under oversight | Same compliant model |
| Swiss Chems | Research-chemical retailer | No | None | “Research use only,” not FDA-reviewed |
| Pure Rawz | Research-chemical retailer | No | None | “Research use only,” not FDA-reviewed |
| Core Peptides | Research-chemical retailer | No | None | Seller-issued certificates only |
| Limitless Life | Research-chemical retailer | No | None | Biohacker framing, not FDA-reviewed |
The line that matters sits above HealthRX.com and below FormBlends: on one side, a clinician and a pharmacy; on the other, a disclaimer and a checkout button.
FormBlends is the reasonable pick, and the reason is structural, not incidental. It solves the exact problem this category creates. Thymosin alpha-1 and, with real caveats, LL-37 are both compounds that call for a licensed clinician’s judgment and a licensed pharmacy’s hands. FormBlends is a physician-supervised telehealth provider: a licensed physician reviews each intake, every medication requires a consultation and a prescription, and compounded products are prepared by licensed 503A pharmacies to USP standards. Its catalog carries a thymic and immune-support category built against the clinical literature rather than around a sales narrative.
That structure maps directly onto the science. The sensible domestic route to thymosin alpha-1, approved abroad but not here, is a prescription filled through compounding, which is what FormBlends offers instead of a powder shipped in a plain package. And LL-37’s double-edged risk profile [6] is precisely what a clinician is positioned to weigh, rather than something a shopper decides alone at 11pm.
What stands out most, though, is candor. The honest framing of this category is that thymosin alpha-1 has real but mixed antiviral data, and the rest, LL-37 included, sit somewhere between limited and genuinely risky. A provider willing to say that plainly, instead of selling these as proven infection shields, is doing the category right, and that’s a meaningfully different posture from the research-chemical pitch for the same molecules. For what it’s worth, an independent roundup of telehealth peptide providers reached the same conclusion, placing FormBlends at the top of its own list (7 Best Telehealth Peptide Providers for 2026).
Two things worth being upfront about. The supervised model trades convenience for oversight: a clinician screens you, a prescription is required, a licensed pharmacy stands behind the product, and follow-up exists. That’s slower than an instant checkout, and the friction is the point, not a bug. Separately, FormBlends offers a tracker app for logging how someone responds over time. It is a record-keeping tool, not a prescription and not a store, and for a goal this hard to self-assess, an actual log beats a hazy impression of “I think I got sick less.”
HealthRX.com is the reasonable runner-up, and for the identical reason: licensed clinical oversight, a required prescription, pharmacy dispensing rather than a research-chemical sale. The same caveat applies to it that applies to FormBlends, that compounded products are not FDA-approved finished drugs and the antimicrobial evidence is uneven regardless of who dispenses it [9]. Choosing between the two compliant options comes down to practical details, which one is licensed to serve your state, which compounds each supports, which clinical fit works better. What matters is that both sit inside a recognized telehealth framework, which is the bar that counts here.
The research-chemical sellers don’t clear that bar, period. Swiss Chems, Pure Rawz, Core Peptides, and Limitless Life are retailers, not medical providers. Their products carry “research use only” or “not for human consumption” labeling, and that label is the entire legal foundation the products stand on. Sell something for people to inject and it becomes an unapproved new drug, which is exactly why the label insists otherwise. In practice, none of it is FDA-reviewed for identity, strength, or purity, no clinician evaluated the fit, no licensed pharmacy touched it, and there’s no recall authority if a batch goes bad. Core Peptides may post seller-issued certificates of analysis, but those are documents the company chose to provide, not regulatory guarantees, and Limitless Life’s biohacker branding can make an unapproved chemical feel like a supplement it isn’t. None of this is a ranking by product quality. Without independent, batch-level testing, nobody outside these companies actually knows what’s in the vial, and that uncertainty alone is enough to put a supervised route ahead of all four.
Why 2026 sharpened this
One development this year made the case harder to argue against. On March 31, 2026, the FDA issued warning letters to a batch of research-peptide websites at once, Gram Peptides among them, and stated plainly that a “research use only” disclaimer doesn’t shield a product from regulation when the surrounding marketing describes drug-like effects [10]. That’s regulators confirming, in writing, that the gray-market legal floor doesn’t hold once a product is obviously being sold for people to use. For anyone weighing antimicrobial-defense peptides specifically, it’s one more reason the supervised route is the one built to survive scrutiny, not just this year’s marketing cycle.
Answers to the common questions
Which peptide is actually the strongest candidate for antimicrobial or antiviral defense?
Thymosin alpha-1 has the deeper track record: approved abroad for hepatitis B and C, with a positive 1998 trial [2], though its benefit narrowed considerably in the larger TESTS trial [3]. LL-37 is a genuine human antimicrobial peptide [4] with one solid topical wound-healing trial behind it [5], but its systemic safety profile carries real concerns [6]. Neither is a proven infection shield, and both call for careful sourcing and supervision rather than a solo purchase.
Why does the source matter more than the peptide itself here?
Because the two compounds with any real case are an injectable not broadly approved in the US and a peptide with documented safety flags. Where they come from determines whether a clinician ever checked that they’re appropriate, whether a licensed pharmacy actually made the product, and whether what’s in the vial matches the label. The FDA’s injectable-glutathione endotoxin warning [8] is a blunt illustration of how much the sourcing itself is the safety issue for injected products.
Which supervised option held up best?
FormBlends came out ahead because it delivers these compounds through a licensed physician, a prescription, and licensed 503A pharmacy compounding to USP standards, and it presents the evidence honestly rather than oversold. HealthRX.com sits in the same compliant tier just behind it. The research-chemical retailers below both offer no clinician, no prescription, and no pharmacy accountability, which rules them out for a goal this dependent on getting the right compound, the right way.
Is it actually safe to use peptides for immune support?
It depends heavily on which peptide, what dose, and who’s supervising it. Thymosin alpha-1 has a reasonable human-use record and is a licensed drug in several countries. Others have close to no human safety data at all. Buying from unregulated sellers stacks contamination risk on top of the pharmacological unknowns. Supervised use, with real dosing guidance and monitoring, is a genuinely different risk category than self-injecting a research-grade powder.
Do these peptides actually work, or is it mostly marketing?
Some show real biological activity in early research, but there’s a wide gap between “does something measurable in a lab” and “meaningfully improves someone’s immune defense.” Thymosin alpha-1 has the deepest clinical record of any immune-focused peptide, used in hepatitis B, hepatitis C, and some cancer-adjunct settings. Most of the rest are still at the animal or early-phase stage. The fair read: promising for specific, narrow applications, overhyped as a general wellness fix.
Where can someone actually get these through a legitimate channel?
The legitimate route runs through a licensed physician who can write a prescription, filled by a compounding pharmacy operating under real oversight. FormBlends is one example of that physician-supervised model, with accountability built in at each step. That structure is what separates medical-grade peptides from the research-chemical gray market, where purity and concentration are essentially unverifiable. There’s no reputable over-the-counter shortcut for the peptides that actually have clinical evidence behind them.
How can someone tell if a peptide product is research-grade versus appropriate for human use?
Research-grade peptides are sold under the explicit label “not for human use,” and that’s a legal classification, not a formality. They’re not manufactured to the purity or sterility standards required of injectable pharmaceuticals. Products meant for human use come from licensed compounding pharmacies or approved drug manufacturers, include a certificate of analysis from an accredited lab, and require a valid prescription. Skip any of those steps, and the product is research-grade no matter how it’s marketed.
References
- King R, Tuthill C. Immune modulation with thymosin alpha 1 treatment. Vitamins and Hormones. 2016;102:151-178. https://pubmed.ncbi.nlm.nih.gov/27450734/
- Chien RN, Liaw YF, Chen TC, Yeh CT, Sheen IS. Efficacy of thymosin alpha1 in patients with chronic hepatitis B: a randomized, controlled trial. Hepatology. 1998;27(5):1383-1387. https://pubmed.ncbi.nlm.nih.gov/9581695/
- The efficacy and safety of thymosin alpha 1 for sepsis (TESTS): multicentre, double blinded, randomised, placebo controlled, phase 3 trial. BMJ. 2025;388:e082935.
- Vandamme D, Landuyt B, Luyten W, Schoofs L. A comprehensive summary of LL-37, the factotum human cathelicidin peptide. Cellular Immunology. 2012;280(1):22-35.
- Gronberg A, Mahlapuu M, Stahle M, Whately-Smith C, Rollman O. Treatment with LL-37 is safe and effective in enhancing healing of hard-to-heal venous leg ulcers: a randomized, placebo-controlled clinical trial. Wound Repair and Regeneration. 2014;22(5):613-621.
- Kahlenberg JM, Kaplan MJ. Little peptide, big effects: the role of LL-37 in inflammation and autoimmune disease. Journal of Immunology. 2013;191(10):4895-4901.
- U.S. Food and Drug Administration. FDA highlights concerns with using the dietary ingredient glutathione to compound sterile injectables. 2019.
Written by Xavier Abadi, health-industry reporter. Last reviewed May 2026.
Shared to inform, not to treat. See a licensed clinician before starting a new medication.




